
We just got back from Hell-ville! Which is just as hot, but much more pleasant than the name might suggest.
Hellville is in fact a port town on the beautiful Island of Nosy Be where we just finished the last leg of a 3 week trip, running training with operating room teams in 3 different hospitals in the north west region of Madagascar. The team have become accustomed to long dusty road trips, but this particular journey culminated with a 45 minute bumpy speedboat transfer over the open ocean, which was rather ‘exciting’ for those in our team who can’t swim!

View from meeting room, Hellville, Nosy Be. Not bad.
Thankfulness for stuff starting with F.
We arrived back to Antananarivo on Thursday, with impeccable timing as it turns out. It was the evening of Thanksgiving, and Kathy, our host at the Mercy Ships team house is American, extremely hospitable, and a fantastic cook.
So with an assembled group of people passing through from America, Australia, Madagascar, South Africa and the UK we took the opportunity to benefit from Kathy’s culinary genius and remember the things we have to be thankful for. The first things that came to mind probably wouldn’t surprise you:
- Firstly, Food (of course, given the setting. Especially pumpkin pie.)
- Friends.
- Family. And another particularly astounding F…
- Free healthcare.
More specifically, free, safe, accessible healthcare. One of the incredible privileges of my life has been to work as a doctor in the UK National Health Service, where care is free at the point of need. Anyone coming to the hospital looking for help will get the best treatment my colleagues and I can give. How much the patient can (or can’t) pay doesn’t even come into it. In a global context, this is truly an extraordinary and rare privilege.
By contrast, 5 billion people in the world do not have adequate access to safe anaesthesia and surgery. They may live many miles away with limited transport. The cost of hospitalisation can prove financially ruinous, and even if you manage to reach a hospital, there may not be the medication, equipment, or expertise available to safely treat you.
So one of the things I have become extremely thankful for is living and working on a part of this map which is comparatively speaking, ‘peachy’.
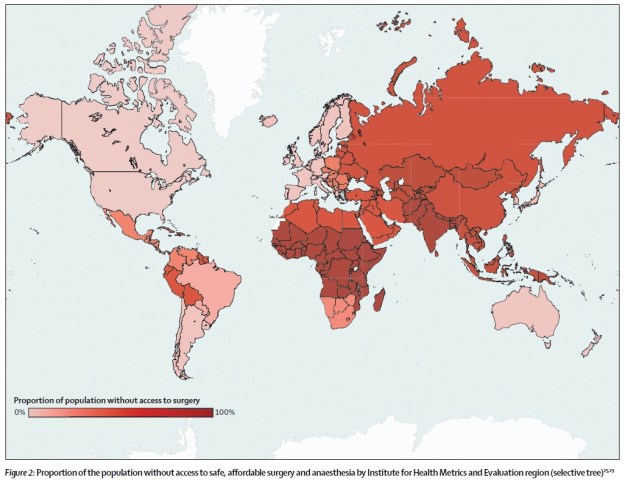
This is a map from the Lancet Commission on Global Surgery published this year(1). It shows the proportion of people in each country worldwide who do not have access to safe, affordable surgery as defined by international standards. The reasons for these geographical disparities are obviously multifaceted and complex, but many people are working hard to see quality and access to services strengthened in those dark red areas.
Isn’t surgery just too expensive?
Surgical services are sometimes perceived as an expensive specialist service, which can only be expected by the privileged few in resource poor settings. Surely providing surgery is just too difficult and costly when money is short?
Far from it! Recent publication ‘Essential Surgery'(3) is part of a comprehensive review and analysis of the most effective (and cost-effective) approaches to global health, produced by the World Bank.
“[This publication] dispels the myth that surgery is too expensive by showing that many essential surgical services rank amongst the most cost-effective of all heath interventions” – Dr Paul Farmer
So where to start? How can you improve the safety of surgical services? Another key conclusion from ‘Essential Surgery’ is that implementing the WHO surgical safety checklist (a simple system for team communication) is affordable, feasible and has been shown to improve safety and quality. This tool simply requires a brief pause to ask some critical questions as a team: firstly before starting anaesthesia, secondly before the knife is put to skin, and finally before the patient leaves the operating room. Simple! Yet remarkably….
“Using the checklist is the best way to reduce surgical errors and improve patient safety.”
– Dr. Margaret Chan, Director-General of WHO

Dr Hasina (centre, blue scrubs) Dr Nandi (far right) with Nosy Be team
This is why we are so excited to be working with the Minister of Health for Madagascar to implement the checklist in all regionals of Madagascar. It is also why Dr Nandi and Dr Hasina (the two extraordinary Malagasy doctors on our team) are so passionate about the opportunity that implementing the WHO Checklist in every region gives for improving healthcare services across Madagascar.

Dr Nandi volunteers as a patient for simulations using the checklist!
How does using a checklist make surgery safer?
A fascinating question! For a full, entertaining and educational answer, I’d recommend Atul Gawande’s best-selling book ‘The Checklist Manifesto’. But specifically, here are two examples of what we do in our training.
Reduced Infections:
According to the WHO, rates of care-associated infected can be up to 20 times higher in developing countries(3). The WHO Checklist we are introducing across Madagascar includes checks to ensure antibiotics are given in a timely fashion, that equipment is properly sterilised, and that no swabs or surgical instruments are accidentally left inside the patient by using rigorous counting techniques. Research consistently shows using the checklist is associated with 50% reduction in post-operative infection and 25% reduction in the need for re-intervention.
Detecting and treating low oxygen levels:
7 in 10 operating rooms in sub-saharan Africa have no pulseoximeter available to monitor oxygen levels during surgery. Without this essential equipment, anaesthesia becomes an intrinsically unsafe process. Consequently, death rates during surgery are between 100 to 1000 times higher in some developing countries than in the developing world (4). We train theatre staff in pulseoximetry use, teach on how to manage falling oxygen levels, and provide Lifebox pulse oximeters for every operating theatre.
‘If anaesthesia providers can correctly interpret the information displayed by an oximeter and respond effectively to treat the cause of hypoxia and prevent it from worsening, many patients who might otherwise die during anaesthesia and surgery will be saved.’ – Global pulseoximetry project

The team using Lifebox pulse-oximeters and documenting surgical counting during a simulated case in the operating room.
Don’t know what you’ve got til it’s….
This might all seem a million miles away from you, especially if you are lucky enough to live in the ‘peachy’ parts of that map.
As I mentioned at the start, November is a month for Thanksgiving. November is also the month for Remembrance Day. I don’t remember life before the NHS, but if you have a few minutes to listen to someone who DOES, 91 year old World War II veteran Harry Leslie Smith’s eloquent and passionate speech in the video at the end of this post moved me to tears when I watched it in 2013. (Disclaimer. It happens it was recorded at a Labour party event, but this is non-party political!)
As well as a debt of gratitude for the enormous cost with which Harry and his colleagues won the freedom I now enjoy, he powerfully reminds us of something else he fears my generation will forget.
‘Poverty and no health care were the norm for the Britain of my youth. That injustice galvanized my generation to become, after the Second World War, the tide that raised all boats.’
After a ‘long hard Great Depression, and a savage and brutal war’, Harry’s generation supported the creation of the NHS. Now, he says his greatest fear is that my generation will allow it to fall by the wayside. I share his concern. At home this month, an overwhelming 98% of junior doctors voted in support of the first all-out industrial action in 40 years in response to the government’s threat to impose contracts for NHS workers which are unfair, unsafe, and have made 7/10 junior doctors consider leaving the NHS. This, despite the fact that the think-tank Nuffield Trust has said that 47,700 more nurses and 26,500 more doctors are needed to match the average for similar countries. This extra staff would cost the NHS another £5bn a year. According to the Organisation for Economic Co-operation and Development (OECD) report of 30 developed countries, while access to care is good in the NHS, the quality of care is suffering after 6 years of under-funding.(5)
Britain has the world’s 5th largest economy.
72% of Britons think the NHS should continue to provide all drugs and treatment at any cost.
Yet only 38% are willing to pay more tax for it.(6).
Wherever you live and work, the question of how we continue to improve affordability, accessibility, and quality of healthcare is one that none of us can afford to ignore. I hope the events at home in the coming weeks will unite the British public around their NHS and it’s incredible staff.
Because too often, we don’t know what we’ve got til it’s gone.
Aneurin Bevan, Minister for Health who established the NHS
(1) Lancet Commision on global surgery executive summary
(2) http://dcp-3.org/volume/34/foreword
(3)WHO Safe Surgery Saves Lives. 10 facts on patient safety. Retrieved 14 Nov 2012
(4) Global pulseoximetry project www.who.int/…/1st_pulse_oximetry_meeting_backgr…
(5) http://www.oecd.org/health/health-at-a-glance-19991312.htm
(6) Economist ‘Physician, heal thyself’ http://www.economist.com/news/britain/21676793-jeremy-hunts-battle-junior-doctors-exposes-awkward-truth-britons-do-not-love
