Are you one of those people? I’m certainly not, but I shared a flat for 4 years with two people who definitely are. You know of whom I speak, the kind of people who quietly take note of an offhand comment mentioning your favourite childhood movie, and months later present you with the limited edition DVD for your birthday. Another friend observed my geekish interest in neuroscience and my love of music making, and thoughtfully gave me a copy of Daniel Levitin’s fascinating book Your brain on music. A gift certificate to spend a day learning to drive a steam train would probably not top the internet search engine suggestions of gifts ‘for her, aged 20s-30s’, but this enjoyable experience courtesy of another friend resulted in the local Steam Museum offering me a position as volunteer train driver. Apparently I have a ‘feel for steam’. I might put that on my CV. In other words, some people seem adept at perfectly matching a gift to what that particular person ACTUALLY wants or needs.
If you are not one of these eerily insightful and thoughtful individuals, it can be much harder to get gifts right, as the survey of 2,000 people for classified ads site Gumtree.com testifies. They found that the UK spent £2.4 billion on unwanted Christmas present in 2011. Only 2% of these gifts are thrown out, and a third end up gathering dust in storage because we feel too bad getting rid of them. (1)
Charitable donations can be similarly tricky. Generosity and good intention are the vital starting point, but by no means the whole story. In 6 months travelling around hospitals in Madagascar, I lost track of the number of pieces of fancy but non-functioning equipment gathering dust in corners. Many were donations, gratefully received but quickly becoming useless in the context to which they had been donated. The WHO once estimated that in lower income countries, up to 80% of equipment in hospitals is donated. This means that local maintenance contracts or supplies are unusual, and assessments show that almost 40% of donated equipment is out of service. (2,3)
One memorably day in the operating room, our scrubs drenched through with sweat in the 35 degree heat, we asked about the air conditioning unit in the corner. It had been donated last year, but stopped working just 3 days later. With no biomedical technician for miles, no one was able to fix it, and it had lain dormant ever since.
Visiting a sick baby on oxygen therapy, we were pleasantly surprised to see the first neonatal resuscitation station we had come across, until we were told it hadn’t been functional for over five years.
A modern and sophisticated ventilator in another hospital also was not being used, as the intermittent and poor quality power supply in the hospital had totally fried the complex circuitry, and no replacement parts were available.
Square peg, round hole
As an anaesthetist in the NHS, I often take for granted the incredible machines that we use daily to deliver a modern miracle of medicine. It is quite astonishing that it is possible for someone to remove one of your internal organs while you are safely kept unconscious with a carefully balanced kind of ‘temporary medical coma’ – general anaesthesia, all the while your vital organ systems are constantly monitored and supported to keep you safe. The anaesthetic machines and monitoring equipment produced in recent years utilise increasingly sophisticated computer processing, and are reliant on infrastructure such as tightly regulated pressurised pipeline gas and uninterrupted electricity supplies. Just a few years ago, ‘A survey conducted among anaesthetists in every African country that has a national society of anaesthesia found only five teaching hospitals in the entire continent that claimed to have good quality supplies of both electricity and oxygen. (2)’ The modern machines mass-produced for our high-tech context are therefore virtually useless and prohibitively expensive in the many parts of the world.
It is no surprise then, that
in 2008, two thirds of the world’s population purchased just 4% by value of the global output of anaesthesia machines. The remaining 96% of mainstream production cannot even be used in most of the places where those 4.5 billion people live. (3)
The equipment developed, used, sold, or donated in resource-rich settings is essentially ‘not fit for purpose’ in the challenging environment of many hospitals around the world, and can even cause waste of valuable resources. This is why organisations like the WHO and AAGBI produce guidelines for anyone seeking to give medical donations.

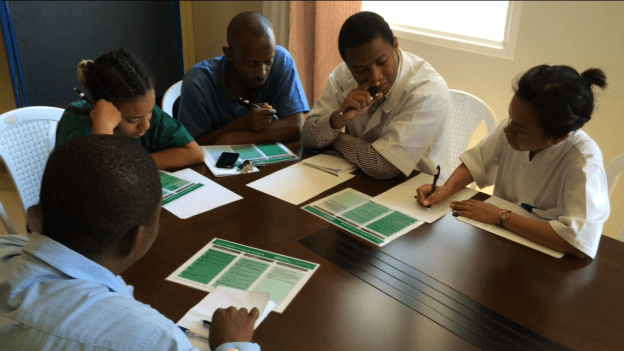
For exactly these sorts of reasons, I was delighted to join a teaching session run by the Medical Capacity Building team from Mercy Ships with members of the anaesthetic team in Hopital Be, Tamatave. UK anaesthetist Steve Alcorn is seen in the picture below, explaining how to use the elegantly simple ‘Glostavent’ anaesthetic machine in the newly refurbished operating room where the team practice running through essential pre-use checks. Just like the Lifebox pulse oximeters our team donated nationwide, the ‘Glostavent’ and the ‘Universal Anaesthesia Machine’ are examples of innovations in equipment technology driven specifically by the needs of underserved populations delivering healthcare with limited resources. The machines are specifically designed to be affordable, durable, and suitable for use in harsh and unpredictable working environments. There is a backup power supply if electricity cuts, and oxygen is extracted directly from the air by the oxygen concentrator.



We have all probably given something to someone else (for the lack of a better more inspired idea!) on the basis that it is what we ourselves would want. Thankfully, in many situations, such a gesture of magnanimity will be appreciated and gratefully received. It’s just as well that with personal relationships it often truly is ‘the thought that counts’!
However in practical matters solutions for provision of global health care, it’s a challenge to find ways to truly understand the needs of a different context instead of just inappropriately transplanting solutions from our own.
‘People trained to do research are concentrated in higher-income regions. The UN Educational, Scientific, and Cultural Organization (UNESCO) estimates that only 13% of the world’s scientists are located in Africa, Latin America, and the Middle East.The highest volume of surgical research is not done in, or by, the countries with greatest clinical need.’ – Global Surgery 2030: Lancet Commission.
This is part of the reason why international collaboration and innovation in this area is essential. Innovation in technology and other areas not only provides increased access to more comprehensive and safe health services for those who desperately need it, but the lessons learned from puzzling out how to provide excellent services when resources are limited may well prove valuable to all of us facing rising health care demands and financial constraint.
I have to admit though, you may still receive novelty socks, bad jumpers, and generic chocolates as Christmas presents. I myself will gratefully receive all of the above.
If you are interested in donating to tried and tested innovative technology being supplied to lower income countries, check out the links below. Thanks for reading!
- Lifebox: Oxygen monitors developed for distribution to every operating room in the world.
- Safe Anaesthesia Worldwide: Charity supporting provision of anaesthetic equipment including appropriate anaesthesia machines worldwide, committed to also providing appropriate training and technical support.
- Great short video on this topic below produced by Tropical Health Education Trust (THET)
Notes: